

Reliant utilizes a secure website to send and sign hiring paperwork. See the steps below for details about how to fill out the forms. The forms you receive will vary depending on your hiring status and work location. This is a general overview, please ask your liaison if you have any detailed questions about your paperwork.
Receive your digital paperwork in an email and click "view document" to open the forms in a web browser
This email contains 2 additional links to forms that you will need to complete from the Field Manual including the Release of Personal Information/Emergency Contact Form.; Release of Personal Information . Please make sure this form is completed & submitted when you do your New Hire Paperwork.

SignNow will open your web browser & tell you how many places you will need to sign on the forms. Here you will click "get started" to start completing the required forms.

The first time you select "Sign" on the form, you will need to select a signature design. You can choose one of their fonts or draw your own.
Fill out each form included in your link. Here is a list of possible forms. Click on the form title below for details and tips on filling out that form. Please follow these guidelines for filling out all forms:
- Red text boxes are required fields and must be completed before submitting
- Once you have completed each box, it will turn green to know it has been completed
- Other text boxes may not be required but you may need to complete them for your hire to be correctly processed
- Read each text box carefully to ensure you type in the correct information
- Manually type into the text boxes as auto-fill features usually cannot determine the correct fields and do so incorrectly
- Use your full legal name as it appears on your Social Security Card
- By signing and submitting these forms, you are verifying that all information is correct to the best of your knowledge according to your current situation and allowing Reliant to process your hire according to the information on these forms.
- Some changes can be made after these forms are submitted. Please see the details on each individual form for when and how to make changes.
This federal tax form directs Reliant on how to handle Federal tax withholding on your paychecks. Below is an example of a filled-out Federal W4 form with instructions.
Please remember to open your PAYSTUB emailed to you each month and review the amount being withheld for your taxes so that you can make adjustments to your chosen W4 options as needed. A new W-4 can be submitted at any time by following the directions on this page: Tax Info & Forms (Link to Federal W4). There is also an option to request a one-time tax adjustment (which may be the case when receiving a bonus where the additional income could cause the tax withholding percentage on your paycheck to be higher than normal.
STATE TAXES:
If you live in a state with income taxes, you will also receive a state tax form to complete. Reliant will default to using the home address of the employee as the working address for state and local income tax withholding. However, in the case of those in a fixed term residency/internship, it is assumed that the employee will spend most of their time at the church/ministry partner location (rather than working from home), so the city and state of that church/ministry partner will be used for tax withholding purposes.
Some states also have local taxes for municipalities and school districts as well as other types of state taxes such as transit taxes, paid leave, or unemployment taxes. Reliant only withholds local taxes when the local jurisdiction or state requires employers to withhold. Local taxes that are optional for the employer to withhold will not be withheld by Reliant and are the responsibility of the employee to report and file on their own behalf.
If an employee moves to a new state or plans to work in another state for more than a month, the employee bears full responsibility to notify Reliant of a move or change in tax withholding location within 2 weeks of the move. If the employee does not report their address change within 2 weeks, causing an incorrect tax location to be used with payroll, the employee will be personally responsible to correct and file their reported wages and taxes to the proper states/local areas on their annual tax filing and pay all associated taxes, penalties, and fees for the corrections. See Tax Info & Forms (Link to Federal W4) for more information.
In general, the W4 form is designed to withhold less taxes than in previous versions of the W4 form. The amount withheld for federal taxes on our paycheck will depend on the options you choose on this form, which we have outlined below. Reliant is only allowed to educate employees on what happens with the options that they can choose. If you have questions, please seek the advice of a tax consultant before your first paycheck.
Below is a list of possible options to choose when submitting a W4:
- Option 1) - select married filing jointly. IMPORTANT: This option assumes that the other spouse is not working and uses the full amount of the standard deduction for 2 people which typically results in a lower amount of taxes withheld. For example, if both spouses work, choosing this option alone option 1 (married filling jointly) without checking the box for multiple jobs/spouse works (see Option 2 below) will result in doubling the standard deduction amount used for calculating taxes withheld on each spouse's paycheck. This will typically result in very little taxes (if any) being withheld, potentially leaving a married couple with taxes due at the end of the year.
For married couples, these options below will, in most cases, ensure a higher amount is withheld:
- Option 2) -select married filing jointly and also check the box “multiple jobs/spouse works”. This option assumes two working people filing taxes with 2 incomes (both spouses working does not mean they both have to be working for Reliant) and this option can also be chosen if you have multiple sources of income.
- Option 3) -select the first box single/married filing separately. This does not affect how you will file your taxes at the end of the year, it is merely for the software to know how much taxes to withhold, which in this case would be based on the standard deduction for 1 person.
- Option 4) - select an option above (single/married filing jointly/multiple jobs) and then under section 4C add a specific monthly dollar amount of extra withholding for federal taxes that you would like Reliant to withhold from each paycheck, which will be added to the amount being withheld out of the paycheck each month based on the type of standard deduction you choose in the top section of the form. This helps to ensure that a specific minimum amount is withheld monthly. However, please note that with this option, this tax amount will be deducted from every payment that is sent from Reliant, including separate backpay checks. Commissioned/Ordained Ministers may choose to utilize this box to indicate an amount they want withheld as extra Federal taxes that they will use to cover their 15.3% SECA (Social Security/Medicare) obligation, since Reliant does not withhold FICA taxes for these employees. See Paying SECA Taxes.
If claiming dependents (on STEP 3 of the form), the W4 deducts a $2000 credit from your total tax withholding for each child. Therefore, if the desired outcome is to have your paychecks withhold federal taxes, you may choose not to elect this dependent credit on your W4 form as it could result in little to no federal taxes withheld. Not claiming dependents on your W4 does not affect your ability to claim your dependents and receive those credits on your yearly tax filing.
REMINDER for dually employed couples:
Married couples where both spouses are employed by Reliant are still treated as two separate employees for taxation purposes. Even though spouses share a fund number, each spouse is paid on a separate check and has taxes withheld on their individual paychecks unrelated to what their spouse chooses for tax settings.
Step 1: Enter Personal Information

Section (a) - please fill in the appropriate information requested for each box. Be sure to double check your data entry for accuracy.
- First name and Middle Initial
- Last Name
- Address
- City
- State
- Zip Code
Section (b)
- Social Security Number
Section (c)
- Select ONE box that best describes your Federal tax filing status
- Single or Married filing jointly
- Married filing jointly (please read info box above, additional steps may apply)
- Head of Household (see instructions before selecting this box)
Steps 2, 3, and 4 below are optional but may be helpful depending on your tax situation. Select items that apply to you to help our system better estimate your federal tax withholding amount. If the below additional options do not apply, proceed to Step 5: Signature
Step 2: Multiple Jobs or Spouse Works

- If you (1) hold more than one job at a time, or (2) are married filing jointly and your spouse also works, you may choose to check box (c) if there are two jobs total for your household and if those jobs are similar in pay. Otherwise, you may elect to leave this box unchecked.
- Note: Reliant cannot advise you on this selection so please make sure you read the instructions carefully and seek outside professional tax assistance if needed.
Step 3: Claim Dependents:
If claiming dependents, the W4 deducts a $2000 credit from your total tax withholding for each child. Therefore, if the desired outcome is to have your paychecks withhold federal taxes, you may choose not to elect this dependent credit on your W4 form as it could result in little to no federal taxes withheld. Not claiming dependents on your W4 does not affect your ability to claim your dependents and receive those credits on your yearly tax filing.

- Multiply the Number of qualifying children under age 17 by $2,000
- See example above, 1 child = $2,000
- Multiply the number of other dependents by $500
- See example, enter $500 for a spouse that you claim (spouse doesn't work outside of the home) or for an older dependent like a special needs adult living in your household
- Add the amounts from both boxes above and enter the total on line 3
Step 4: Other Adjustments

4(a) Other Income (not from jobs)
This box may be used to indicate additional withholding you want withheld annually to cover other sources of income on which you will pay taxes, such as retirement income or investment income.
See example above, if I expect to have $1200 in Capital Gains on which I'll owe taxes for the year, you may want to enter that amount in this 4(a) box.
4(b) Deductions
This box may be used to indicate deductions that you anticipate in excess of the standard deduction amount.
See example above, if I expect to have itemized deductions that exceed the standard deduction amount by $5,000, I would enter $5,000 in this 4(b) box.
- Note: If you anticipate taking the standard deduction when filing your taxes, leave this box blank.
4(c)Extra Withholding
- This box may be used to enter additional tax you want withheld each pay period
- Note: Reliant pays monthly so these extra withholding taxes would be withheld every month, in addition to your normal taxes for that paycheck.
- Commissioned/Ordained Ministers may choose to utilize this box to indicate an amount they want withheld as extra Federal taxes that they will use to cover their 15.3% SECA (Social Security/Medicare) obligation, since Reliant does not withhold FICA taxes for these employees. See Paying SECA Taxes.
Requesting EXEMPTION from Federal Tax Withholding

- To claim exemption from federal tax withholding due to Foreign Earned Income Exclusion or other qualified reasons, the W-4 instructions say write “Exempt” in the space below Step 4(c). Then, ensure you have completed Steps 1a, 1b, and 5. There is an "Optional" Box on the form for you to indicate this EXEMPT selection.
- See example above, please Type in "EXEMPT" to elect this tax setting.
- Do not complete Steps 2-4 on the form if claiming exemption.
Step 5: Sign Here

- See example above, by selecting "sign" and entering a digital signature this will complete your acknowledgement/submission of this form.
This form contains detailed information about the terms of employment with Reliant.
Signature

- Please read the entire text
- By selecting "sign" and entering a digital signature along with typing in your 4-digit MTD FD# this will complete your acknowledgement/submission of this form.
This form may be included for Reliant employees serving in the United States who are benefits eligible. If you need to make any benefits selections before your hire, please email benefits@reliant.org.
Section A: Select from the drop down at the top. If enrolling in coverage complete with general information about yourself in the blue boxes.
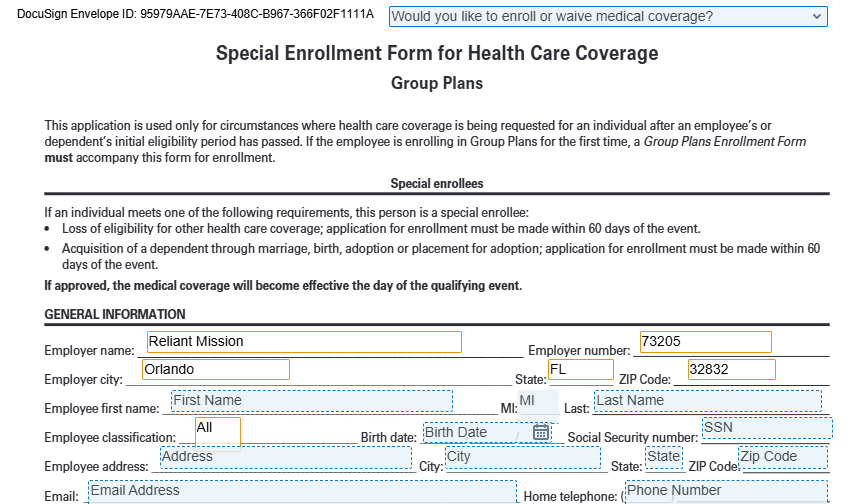
Section B: If you are enrolling in coverage select who you are enrolling in coverage.
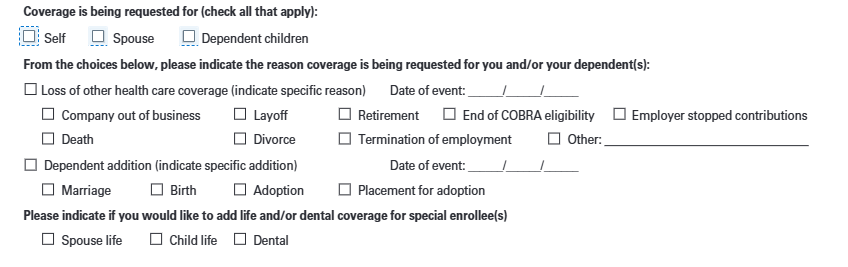
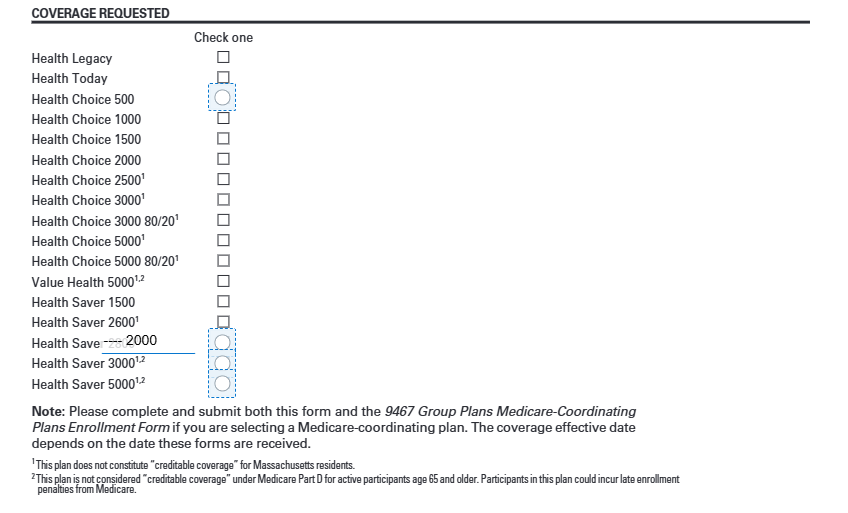
Section C: Select what plan you are enrolling in.
Section C : If are enrolling in coverage, complete this box with who will be on your plan. Then it will take you to Section E to sign and submit.

Section D : If you are waiving medical coverage
- Fill out the information in the blue boxes.
- Select who you are waving coverage for
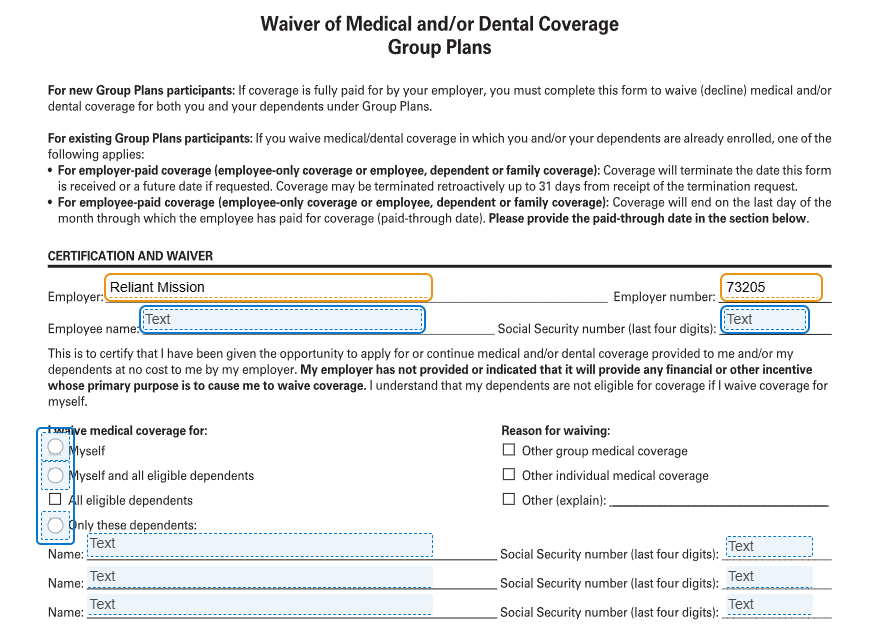
Section E : Sign the form.
This form may be included for benefits-eligible Reliant employees serving in the United States. Dental coverage is an optional coverage that employees may choose to enroll in or decline coverage. See Dental Insurance - Coverage and Rates for additional information about this coverage. If you need to make any benefits selections before your hire, please email benefits@reliant.org.
Enrolling in/Declining Voluntary Dental Coverage:

Select from the Drop Down menu options:
- "I want to enroll in dental coverage."
- "I DO NOT want to enroll in dental coverage."
- The drop down box will remain blank but your selection will allow you to skip completion of the form (if declining coverage) or additional red text boxes will appear (if enrolling in coverage)
Enrolling in Dental Coverage

- Select the plan you want to enroll in:
- DENTAL LOW (Tier One "Low" Plan, Dental 1250)
- DENTAL HIGH (Tier Two "High" Plan, Dental 1500)
- Marital Status
- Social Security Number
- Employee's Last Name, First, MI (Middle Initial)
- Date of Birth
- Male/Female
- Occupation: Use Missionary or Pastor etc.
- Hours worked per week
- Are your earnings paid Hourly/Salaried
- Street Address
- City
- State
- Zip
- Question: Are you covered under another Dental Insurance Plan? Yes/No
- Question: Dependents (Are they covered under another Dental Insurance Plan?) Yes/No
- Dependent Coverage information: Fill in Required fields for all dependents being covered on this dental plan
- Full Legal Name (Last, First, MI)
- Select: ADD
- Relationship: Type Spouse or Child
- Sex: M/F
- Date of Birth
- Social Security Number
Signature

- By selecting "sign" and entering a digital signature this will complete your submission of this form.
You will still need to sign the document even if you select not to enroll in coverage.
This form may be included for Reliant employees serving overseas. If you need to make any benefits selections before your hire, please email benefits@reliant.org.


Please follow the instructions below to learn more about what information is needed for each sections.
If you have any questions filling out the Aetna Enrollment Form, please email benefits@reliant.org
Section 1: Policy / Plan Details
This section is to be done by Reliant office staff. Nothing needs to be completed by you at this time.
Section 2: Employee Details
Covered Member Details
This is where you will fill out your personal details. The boxes outlined in red are required and will not let you move forward without completing them.
- Last Name: full legal last name
- First Name: full legal first name
- MI: middle initial (optional)
- Date of Birth: input in Day, Month, Year format (example: 1 January 2023)
- Male / Female: select whichever applies to you

Section 3: Contact Details
Employee Mailing Address
Please input the address where you would like to receive mail.
- Email address: this can be your reliant.org email address or another email address you have access to
- Telephone Number
- Country
- Mailing Address line 1
- Mailing Address line 2 (optional)
- Mailing Address line 3 (optional)
- City
- State / Province (if outside of the US)
- Zip Code

Resident Location
This is the country or location where you are physically present for at least half of a one-year period.
If your Resident Location is the same as your mailing address, you can check the box that says "Check If same as the mailing address."

This will eliminate the boxes, and we will use your mailing address information for your resident location.
If it's not the same as your mailing address, fill out the sections below:
- Country
- Mailing Address line 1
- Mailing Address line 2 (optional)
- Mailing Address line 3 (optional)
- City
- State / Province (if outside of the US)
- Zip Code

Section 4: Additional Information
Citizenship
Please input your primary country of citizenship.
You can add two additional citizenships if desired. If you have more than 2 additional citizenships, please email benefits@reliant.org

Home/origin location
This is the location where the employee resided prior to their assignment and maintains a residence to return to during or following their assignment.
- Country
- City
- State / Province
If your Home/origin Location is the same as your mailing address, you can check the box that says "Check If same as the mailing address."

This will eliminate the boxes, and we will use your mailing address country, city and state for your home/origin location.
Dependents
Here is where you can add dependents if desired.
Boxes will appear, and you can add your dependents. You can add up to seven dependents. If you need more than seven, please email benefits@reliant.org to get them added to your insurance plan.
- Dependent's Full Legal Name
- Dependent's Relationship to you (husband, spouse, daughter, son)
- Dependent's Birth date
- Dependent's Primary Country of Citizenship


Nothing more needs to be done. You can move on to the next section.
Signatures
Sign the document, and adopt the signature if needed.
Then click "Finish" to submit your form.
If you miss anything, the form will require you to complete the red boxes before you can select "finish."

If you see the option to download and print your form, then your form is submitted!

This form may be included for benefits-eligible Reliant employees serving in the United States or overseas. The purpose of this form is to designate beneficiaries for required life insurance coverage with Reliant. See Group Life and Voluntary Life Insurance for more details on this coverage. Beneficiary changes can be mad at any time by submitting a new form according to the information on the previously linked page.
Top Section: Enter your Information

- Insured name: (Your Name) First Name Last Name
- Social Security Number: Your Social Security Number
Middle Section: Enter the Information of your Beneficiaries
Primary Beneficiary

Primary/Contingent Beneficiary
If you want to elect more than one Primary or Contingent Beneficiary, enter their name in the optional box, and the remaining required cells will populate. Remember that the divided percentage must total 100%.
- Full Name and Address: Enter the Full Name (First Name Last name) and Address of the person you are selecting as your Primary Beneficiary
- Percentage: Enter 100% (*see details above if you'd like to name more than one Primary Beneficiary)
- Date of birth: Enter your Primary Beneficiary's date of birth
- Relationship: Enter your Primary Beneficiary's relationship to you - Ex. Spouse, Child, Parent, Friend Etc.
- Social Security Number: Enter your Primary Beneficiary's Social Security Number (if choosing a church/charity, enter the organization's Tax ID Number)
Contingent Beneficiary - This is the alternate beneficiary, used only if the Primary Beneficiary is unable to claim the life insurance payout

- Full Name and Address: Enter the Full Name (First Name Last name) and Address of the person you are selecting as your Contingent Beneficiary
- Percentage: Enter 100% (*see details above if you'd like to name more than one Contingent Beneficiary)
- Date of birth: Enter your Contingent Beneficiary's date of birth
- Relationship: Enter your Contingent Beneficiary's relationship to you - Ex. Spouse, Child, Parent, Friend Etc.
- Social Security Number: Enter your Contingent Beneficiary's Social Security Number
Signature

- By selecting "sign" and entering a digital signature this will complete your submission of this form.
This form may be included for Reliant employees serving in the United States or overseas. This form is ONLY to be filled out if you are electing OPTIONAL voluntary life insurance coverage - See Group Life and Voluntary Life Insurance for premium rates and more details on this benefit. Please note monthly premiums for this elected coverage will be deducted from the employee's paycheck. If you need to make any benefits selections before your hire, please email benefits@reliant.org.
Declining Voluntary Life Coverage:

- Select from the Drop Down menu: "I do not want to purchase additional voluntary life insurance coverage."
Electing Voluntary Life Coverage:

- Select from the Drop Down menu: "I am electing to purchase additional voluntary life insurance coverage."
Employee/Member Information: Complete these fields with YOUR Personal Information

- Name: (Your Name) First Name Last Name
- Social Security Number
- Gender: Male/Female
- Date of Birth
- State of Birth
- Address
- City
- State
- Zip
- Phone Number
- Occupation: Use Missionary or Pastor etc.
- Annual Compensation: Use the annual salary you are accepting from Reliant
- Hours worked per week
- Email address: This should auto-fill
- Question: Are you actively performing the duties of your occupation or profession? Select "Yes"
- Question: Have you used tobacco in any form in the last 12 months? Select the appropriate answer - Yes/No
Coverage Elected and Amounts: Select the Amounts and Types of Coverage from the options provided

Voluntary Term Life Coverage Employee
- This is additional Life insurance to cover you, the employee.
- Select Enroll/Decline per your preference
- Note: you may elect up to $100,000 in guaranteed coverage. For greater amounts of coverage RSLI may seek evidence of insurability. Contact Employment Services for information about this benefit.
Voluntary Term Life Spouse

- This is additional Life insurance to cover your spouse
- Select Enroll/Decline per your preference
- Note: you may elect up to $30,000 in guaranteed coverage. For greater amounts of coverage RSLI may seek evidence of insurability. Contact Employment Services for information about this benefit.
- Once you Select "enroll" for this coverage you will then need to go back and complete the section above titled: Spouse Information (it will appear with red text boxes when you select "Enroll")
- Spouse Name
- Gender
- Date of Birth
- State of Birth
- Address
- City
- State
- Zip
- Question: Has your spouse used tobacco in any form in the last 12 months? Select the appropriate answer - Yes/No
Voluntary Term Life Dependents
- This is additional Life insurance to cover your dependents (children 26 years of age and younger).
- Select Enroll/Decline per your preference
- Note: you may elect up to $10,000 in guaranteed coverage.
Click "finish"

Reliant will review the paperwork and notify you should we need corrections or additional paperwork.
Once the forms have been verified as complete, you will receive an email with all completed forms attached as PDF's.